IVD Protrusions and Extrusions
The successful chiropractic management of large intervertebral disc herniations requires careful consideration. The complex multifactorial factors associated with the genesis, prevalence, clinical presentation, progression, assessment, and non-surgical/surgical interventions are substantial.
Current research indicates that non-surgical care should be exhausted before considering surgical interventions in acute stages of lumbar disc herniation. The potential for clinical degradation represents a significant risk to the patient and attending physicians. Surgical consultation and interventions may be necessary due to neurologic deficits and intolerable pain.
A Macrophage and Lymphocyte Mediated Response
It has been postulated that the spontaneous resorption of herniated disc material is facilitated when it ruptures through the posterior longitudinal ligament and is exposed to the epidural vascular supply. Macrophage and lymphocytes signal a cascade of inflammatory sequelae and neovascularization that produces a collar of granulation tissue around the disc fragment that facilitates resorption.
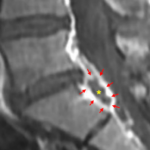
The Bullseye Sign
Contrast enhanced T1 weighted images provide an opportunity to visualize the collar of granulation tissue that has been termed, “The Bullseye Sign.” On the image below, the increased signal intensity is identified by red arrows, surround the herniated disc material that is designated with the yellow asterick.

The Bullseye sign has been associated with an increased likelihood of the resorption of sequestered disc material.
Elements of Predictive Value
The ability to qualify large herniations that are more likely to resorb is beneficial to patient management. Treatment recommendations and planning can be refined with a better understanding of those factors that increase or decrease the likelihood of resorption that include:
- The Bullseye sign.
- Sequestrated disc tissue that is no longer attached to the parent disc and ruptures through the posterior longitudinal ligament.
- Large disc fragments.
- Younger age.
- The absence of Modic 1 changes.
- The absence of endplate cartilage within the sequestrated disc fragment.
Non-Surgical Care
Recent studies indicate that non-surgical interventions should be attempted for large disc herniations and sequestrations, in the absence of neurologic deficits. These interventions may include chiropractic care, traction, physical therapy, medication and spinal injections.
Patients should be monitored regularly in the attempt to protect against condition degradation. In the event of the development of progressive neurologic deficits, patients should be referred for surgical consultation.
For more in depth review of this topic, advanced CE is available at PostGradDC.com.